By Dr Than Lwin Tun
MONKEYPOX is caused by the monkeypox virus which belongs to the orthopoxvirus genus of the Poxviridae family. There are two clades of monkeypox virus: the West African clade and the Congo Basin (Central African) clade. The name monkeypox originates from the initial discovery of the virus in monkeys in a Danish laboratory in 1958. The first human case was identified in a child in the Democratic Republic of the Congo in 1970.
Monkeypox virus is transmitted from one person to another by close contact with lesions, body fluids, respiratory droplets and contaminated materials such as bedding. The incubation period of monkeypox is usually from 6 to 13 days but can range from 5 to 21 days. Various animal species have been identified as susceptible to the monkeypox virus. Uncertainty remains on the natural history of the monkeypox virus and further studies are needed to identify the exact reservoir(s) and how virus circulation is maintained in nature.
Monkeypox is usually self-limiting but may be severe in some individuals, such as children, pregnant women or persons with immune suppression due to other health conditions. Human infections in the West African clade appear to cause less severe disease compared to the Congo Basin clade, with a case fatality rate of 3.6 per cent compared to 10.6 per cent for the Congo Basin clade.
Outbreak at glance
Since 13 May 2022, cases of monkeypox have been reported to World Health Organization (WHO) from 12 Member States that are not endemic to the monkeypox virus, across three WHO regions. Epidemiological investigations are ongoing, however, reported cases thus far have no established travel links to endemic areas. Based on currently available information, cases have mainly but not exclusively been identified amongst men who have sex with men (MSM) seeking care in primary care and sexual health clinics.
The objective of this Disease Outbreak News is to raise awareness, inform readiness and response efforts, and provide technical guidance for immediate recommended actions.
The situation is evolving and WHO expects there will be more cases of monkeypox identified as surveillance expands in non-endemic countries. Immediate actions focus on informing those who may be most at risk for monkeypox infection with accurate information, to stop further spread. The currently available evidence suggests that those who are most at risk are those who have had close physical contact with someone with monkeypox, while they are symptomatic. WHO is also working to provide guidance to protect frontline health care providers and other health workers who may be at risk such as cleaners. WHO will be providing more technical recommendations in the coming days.
Description of the outbreak
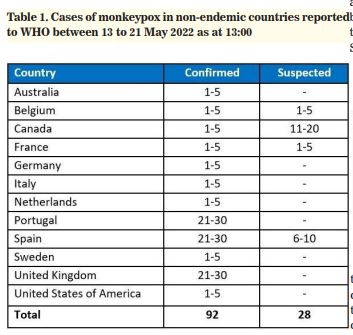
As of 21 May, 13:00, 92 laboratory-confirmed cases, and 28 suspected cases of monkeypox with investigations ongoing, have been reported to WHO from 12 Member States that are not endemic for monkeypox virus, across three WHO regions (Table 1). No associated deaths have been reported to date.
Reported cases thus far have no established travel links to an endemic area. Based on currently available information, cases have mainly but not exclusively been identified amongst men who have sex with men (MSM) seeking care in primary care and sexual health clinics.
To date, all cases whose samples were confirmed by PCR have been identified as being infected with the West African clade. Genome sequence from a swab sample from a confirmed case in Portugal indicated a close match of the monkeypox virus causing the current outbreak, to exported cases from Nigeria to the United Kingdom, Israel and Singapore in 2018 and 2019.
The identification of confirmed and suspected cases of monkeypox with no direct travel links to an endemic area rep resents a highly unusual event. Surveillance to date in non-endemic areas has been limited but is now expanding. WHO expects that more cases in non-endemic areas will be reported. Available information suggests that human-to-human transmission is occurring among people in close physical contact with cases who are symptomatic.
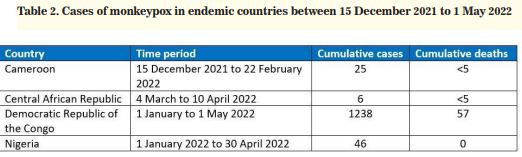
In addition to this new outbreak, WHO continues to receive updates on the status of ongoing reports of monkeypox cases through established surveillance mechanisms (Integrated Disease Surveillance and Response) for cases in endemic countries, as summarized in Table 2.
Monkeypox endemic countries are Benin, Cameroon, the Central African Republic, the Democratic Republic of the Congo, Gabon, Ghana (identified in animals only), Ivory Coast, Liberia, Nigeria, the Republic of the Congo, Sierra Leone, and South Sudan.
Public health response Further public health investigations are ongoing in non-endemic countries that have identified cases, including extensive case finding and contact tracing, laboratory investigation, clinical management and isolation provided with supportive care.
Genomic sequencing, where available, has been undertaken to determine the monkeypox virus clade(s) in this outbreak.
Vaccination for monkeypox, where available, is being deployed to manage close contacts, such as health workers. WHO is convening experts to discuss recommendations on vaccination.
WHO risk assessment
Endemic monkeypox disease is normally geographically limited to West and Central Africa. The identification of confirmed and suspected cases of monkeypox without any travel history to an endemic area in multiple countries is atypical, hence, there is an urgent need to raise awareness about monkeypox and undertake comprehensive case finding and isolation (provided with supportive care), contact tracing and supportive care to limit further onward transmission.
Cross-protective immunity from smallpox vaccination will be limited to older persons since populations worldwide under the age of 40 or 50 years no longer benefit from the protection afforded by prior smallpox vaccination programmes. There is little immunity to monkeypox among younger people living in non-endemic countries since the virus has not been present there.
Historically, vaccination against smallpox had been shown to be protective against monkeypox. While one vaccine (MVABN) and one specific treatment (tecovirimat) were approved for monkeypox, in 2019 and 2022 respectively, these countermeasures are not yet widely available.
Based on currently available information, cases have mainly but not exclusively been identified amongst men who have sex with men (MSM) seeking care in primary care and sexual health clinics. No deaths have been reported to date. However, the extent of local transmission is unclear at this stage, as surveillance has been limited. There is a high likelihood of identification of further cases with unidentified chains of transmission, including in other population groups. With a number of countries in several WHO regions reporting cases of monkeypox, it is highly likely that other countries will identify cases.
The situation is evolving and WHO expects there will be more cases of monkeypox identified as surveillance expands in non-endemic countries. So far, there have been no deaths associated with this outbreak. Immediate actions focus on informing those most at risk for monkeypox infection with accurate information, stopping the further spread and protecting frontline workers.
WHO advice
Identification of additional cases and further onward spread in the countries currently reporting cases and the other Member States is likely. Any patient with suspected monkeypox should be investigated and if confirmed, isolated until their lesions have crusted, the scab has fallen off and a fresh layer of skin has formed underneath.
Countries should be on the alert for signals related to patients presenting with an atypical rash that progresses in sequential stages – macules, papules, vesicles, pustules, scabs, at the same stage of development over all affected areas of the body – that may be associated with fever, enlarged lymph nodes, back pain, and muscle aches. These individuals may present to various community and healthcare settings including but not limited to primary care, fever clinics, sexual health services, infectious disease units, obstetrics and gynaecology, urology, emergency departments and dermatology clinics. Increasing awareness among potentially affected communities, as well as health care providers and laboratory workers, is essential for identifying and preventing further secondary cases and effective management of the current outbreak.
Reference
-WHO factsheet on monkeypox
-WHO monkeypox outbreak
toolkit